Keep Your Uterus and Stop Heavy Periods With an Endometrial Ablation
Uterine-sparing minimally invasive alternatives to hysterectomy. Read more

Uterine-sparing minimally invasive alternatives to hysterectomy. Read more
Here is what pregnant women need to know about Coronavirus. Read more
Are tests accurate, and can we trust the results? Read more
Which side you are on makes no difference to COVID-19. Read more
A small gift from a patient reminds a nurse what matters. Read more
Our little bundle of joy, Mila Sofia, officially arrived on June 22nd, and we are so incredibly in love. Read more
Understanding the mystery of the mammary glands.
We all have breasts. Structurally, breasts are simply modified sweat glands. But functionally, the mammary glands produce milk, life- saving nutrition for newborn babies allowing the human race to evolve and flourish.
The mammary glands are wondrous and complex structures. Let’s take a tour of the breast anatomy.

Used with permission from Medika Life
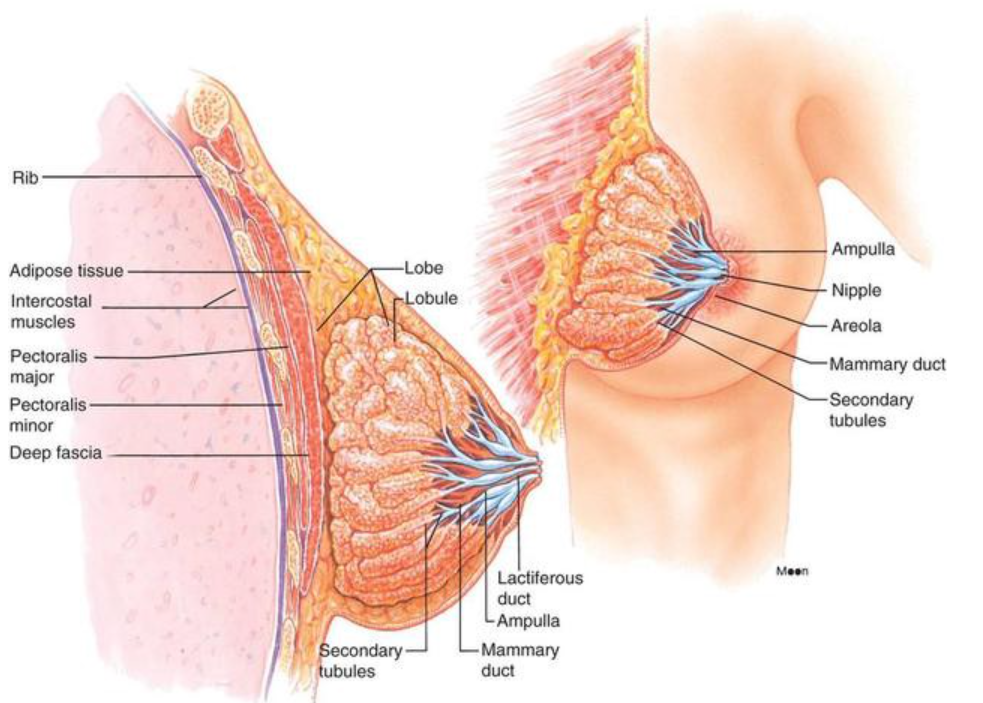
Mammary glands are located in the breast overlying the pectoralis major muscles. Both males and females have them, but they are functional only in women.
Externally, each breast has a raised nipple surrounded by a circular pigmented area called the areola. The nipples are sensitive to touch because of a dense array of nerve fibers and smooth muscle that contracts and causes them to become erect in response to stimulation.
Internally, the adult female breast contains 15 to 20 lobes of glandular tissue that radiate around the nipple. The lobes are separated by firm connective tissue and fatty adipose tissue.
The connective tissue helps support the breast. Bands of connective tissue, called suspensory (Cooper’s) ligaments, extend through the breast from the skin to the underlying muscles. The amount and distribution of the adipose tissue determine the size and shape of the breast. To keep it simple, fatty tissue determines breast size and connective tissue holds them up.
Have you ever wondered how milk gets to the nipple? Each lobe consists of lobules that contain the milk-producing glandular units. A tube called a lactiferous duct collects milk from the lobules and carries it to the nipple.
Milk is stored in a reservoir called the ampulla (lactiferous sinus) just before arrival at the nipple. After the sinus, the duct splits and narrows allowing multiple ducts to bring milk to the surface of the nipple.
Four hormones have an integral role in breast development. Estrogen levels increase during puberty and stimulate the production of glandular breast tissue. Estrogen increases adipose tissue causing the breast to increase in size. Progesterone plays a role as well by stimulating the development of the duct system.
During pregnancy, these hormones further enhance the development of the mammary glands. Prolactin from the anterior pituitary gland stimulates the milk production inside of the glandular tissue, and oxytocin triggers the ejection of milk from the glands.
Used with permission from Medika Life
The breast is located on the anterior thoracic wall. It extends horizontally from the lateral border of the sternum to the mid-axillary line. Vertically, it spans between the 2nd and 6thintercostal cartilages. It lies superficially to the pectoralis major and serratus anterior muscles.
The breast is composed of two regions. The circular body is the prominent area of the breast. The axillary tail is a smaller area running along the inferior lateral edge of the pectoralis major towards the axillary fossa.
At the center of the breast is the nipple. It is made mostly of smooth muscle fibers. The pigmented area of skin surrounding the nipple is called the areolae. There are numerous sebaceous glands within the areolae . These glands enlarge during pregnancy, secreting an oily protective lubricant for the nipple.
The middle of the breast receives blood from the internal mammary artery, a branch of the subclavian artery.
The lateral part of the breast receives blood from four vessels:
Used with permission from Medika Life
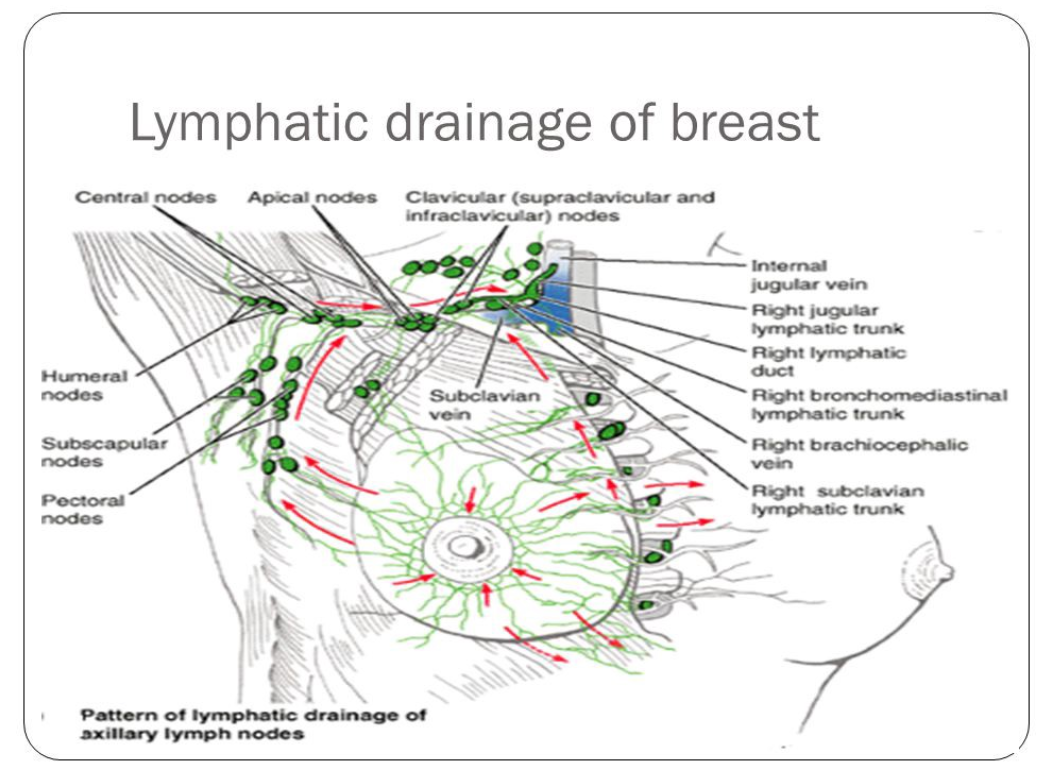
The lymphatic drainage of the breast is incredibly important. Breast cancer spreads through the lymph when it spreads (metastisizes).
There are three groups of lymph nodes that receive lymph from breast tissue — the axillary nodes (75%), parasternal nodes (20%), and posterior intercostal nodes (5%).
Thank you to BeingWell for publishing this article on Medium.
Originally posted on Medika Life
Blog Author: Dr. Richard Wagner
Main Blog Photo By: Jan Kopřiva on Unsplash

Skin care is the key to adolescent acne frustrations.
Facetime, Houseparty, Tik Tok, and Zoom meetings. Our teenagers are always online, and they want their face to look good on screen. One of the side effects of online school and the stay-at-home order is increased concerns about acne.
Our pediatric office has many acne advice requests, as young people notice the skin blemishes in their HI-Def-selfie world.
There are a lot of myths about acne. Your grandmother will tell you its all in the diet. Believe it or not, acne is not caused by eating too much chocolate or greasy food.
Acne breakouts occur due to a combination of factors such as spikes in certain hormones, clogged pores in the skin, and common but mostly mild skin infections.
The best way to prevent acne is to take care of your skin. Clean and healthy skin is more resistant to pimply outbreaks.
1. Wash your face. Use warm water and cleanser specifically designed for the face. Harsh soaps and scrubs may damage the skin and make acne worse.
2. Do not pick, squeeze, or pop pimples.
3. Avoid oil-based skin products and make-up. One easy trick is to choose a moisturizer with the words “non-comedogenic” on the label.
4. Try an over the counter medication.
5. Be skeptical of online and television advertising highlighting magic cures and overnight remedies.

Pimples are so tempting. They stare at you in the mirror, almost begging to be popped. Don’t do it. Resist the urge to squeeze it until it bursts. Pimple popping is one of the worst things you can do as it damages the underlying skin.
Damaged skin can lead to scarring and worsen the skin’s appearance.
At the first sign of an acne breakout of acne is first noticed, you can try over the counter products like salicylic acid and benzoyl peroxide. These products help to clean the skin and remove debris from pores.
It is always a good idea to start off trying a little of these products on small skin areas. Acne medication can cause skin irritation and, occasionally, an adverse reaction.
If these over the counter solutions do not yield positive results, schedule an evaluation with your pediatric healthcare provider for an assessment. There are multiple medications that your pediatrician can prescribe based on the type and severity of acne.
A pediatric appointment either in person or by using telemedicine technology can provide a massive lift in self-esteem, allowing our youth to embrace the prom, graduation, or even their next Zoom gathering.
Thank you to BeingWell for publishing this article on Medium.
Blog Author: Dr. Agboola O. Fatiregun
Main Blog Photo By: dima_sidelnikov Istock by Getty

Understanding how endometriosis affects your health and future pregnancy.
What is the deal with painful periods? Some people suffer every month while others never experience cramps. The most common cause of painful periods (dysmenorrhea) is endometriosis.
Endometriosis happens when tissue similar to the lining of the uterus grows outside of the uterus where it does not belong. It causes painful periods and affects more than 11% of American women. It is especially common among women age 25–35, and may impact ones ability to get pregnant. Several different treatment options can help manage the symptoms, improve your life, reduce pain, and improve your chances of getting pregnant.
Endometriosis, sometimes called “endo,” is a common gynecologic health problem. It gets its name from the word endometrium, the tissue present in the lining of the uterus or womb. For women with endometriosis, this tissue begins growing outside of the uterus and on other areas in the body where it doesn’t belong.
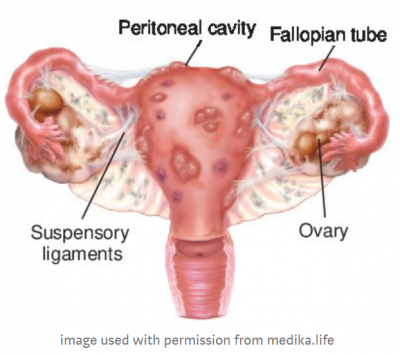
Most often, endometriosis is found on the:
Endometriosis implants may also be found in the vagina, cervix, vulva, bowel, bladder, or rectum. Rarely, endometriosis appears in other parts of the body, such as the lungs, brain, and skin.
Symptoms of endometriosis can include:
Endometriosis growths are benign (not cancerous), but they can still cause troublesome problems.
Remember, endometriosis implants occur when tissue similar to the lining of the uterus begins to grow outside of your uterus where it doesn’t belong. Endometriosis growths may swell and bleed in the same way the lining inside of the uterus does every month during menstrual cycles. This process causes swelling, pain, and scar tissue because the tissue grows and bleeds in an area where it cannot easily get out of your body.
The endometriosis implants may also continue to expand causing problems such as:
Endometriosis is a common health problem for women affecting approximately 11% of women, or more than 6 ½ million women in the United States, have endometriosis. The exact number is unknown as many women who have endometriosis suffer no symptoms at all. Obgyns often discover endometriosis during routine surgeries such as tubal ligations.
Endometriosis can happen to any woman who has menstrual periods, but it is more common in women 25–35 years old. Occasionally, we find endometriosis in young girls before they begin having periods which is called premenarcheal endometriosis.
You might be more likely to get endometriosis if you have:
No one knows for sure what causes this disease. Researchers are studying possible causes:
You can’t prevent endometriosis. But you can reduce your chances of developing it by lowering the levels of the hormone estrogen in your body. Estrogen helps to thicken the lining of your uterus during your menstrual cycle.
To keep lower estrogen levels in your body, you can:
If you have symptoms of endometriosis, talk with your doctor. The doctor will talk to you about your symptoms and do or prescribe one or more of the following to find out if you have endometriosis:
There is no cure for endometriosis, but treatments are available for the symptoms and problems it causes. Talk to your doctor about your treatment options.
If you are not trying to get pregnant, hormonal birth control is generally the first step in treatment. This may include:
The hormonal treatment works only as long as it is taken, and is best for women who do not have severe pain or symptoms.
Elagorix (brand named Orilissa) is a new medication indicated for endometriosis. It works by interacting with the hormones LH (luteinizing hormone) and FSH (follicle-stimulating hormone) to reduce the amount of circulating Estrogen. This medication is highly effective at reducing moderate to severe pain associated with endometriosis
If you are trying to get pregnant, your doctor may prescribe a gonadotropin-releasing hormone (GnRH) agonist. This medicine stops the body from making the hormones responsible for ovulation, the menstrual cycle, and the growth of endometriosis. This treatment causes a temporary menopause, but it also helps control the growth of endometriosis. Once you stop taking the medicine, your menstrual cycle returns, but you may have a better chance of getting pregnant.
Surgery is usually chosen for severe symptoms, when hormones are not providing relief or if you are having fertility problems. During the operation, the surgeon can locate any areas of endometriosis and may burn, destroy, or remove the endometriosis implants. The surgeon may also test to see if the fallopian tubes are open (chromotubation). After surgery, hormone treatment is often restarted unless you are trying to get pregnant.
Other treatments you can try, alone or with any of the treatments listed above, include:
For some women, the painful symptoms of endometriosis improve after menopause. As the body stops making the hormone estrogen, the growths shrink slowly. However, some women who take menopausal hormone therapy may still have symptoms of endometriosis.
If you are having symptoms of endometriosis after menopause, talk to your doctor about treatment options.
Yes. Many women with endometriosis get pregnant. But, you may find it harder to get pregnant. Researchers think endometriosis may affect as many as one in every two women with infertility.
No one knows exactly how endometriosis might cause infertility. Some possible reasons include:
If you have endometriosis and are having trouble getting pregnant, talk to your doctor. He or she can recommend treatments, such as surgery to remove the endometrial growths.
Research shows a link between endometriosis and other health problems in women and their families. Some of these include:
Thank you to BeingWell for publishing this article on Medium.
Article Originally published at https://medika.life on July 9, 2020.
Blog Author: Dr. Jeff Livingston
Main Blog Photo by: Anthony Tran on Unsplash
Happy Father’s Day to our Mac-Dad’s and all the Dad’s!💖 Read more
