

Labor induction methods do not work for everyone, and here’s why.
Inducing labor is not always straightforward and there are several reasons why your provider will recommend one method over another. Obstetric providers induce labor for medical reasons (gestational hypertension, gestational diabetes, poor fetal growth, among many others), elective reasons, or because your pregnancy is post-dates. Whatever the reason, the method for inducing labor is determined by your cervical dilation and past pregnancy history/outcomes.
Before I review the common methods of inducing labor, let me first explain that these methods are used by licensed medical professionals. If you came here for “natural” induction techniques, then you clicked on the wrong article.
Let me just say that if you want to try at-home techniques, please talk to your healthcare provider. We are not opposed to natural methods, but there are side effects/risks that may put certain pregnancies at increased risk. Also, I never, ever recommend castor oil to induce labor. Diarrhea-induced contractions are not the type of contractions you want to suffer through.
Inducing labor can take several hours, if not days, and you may need multiple methods throughout the induction process. Please note the time limits posted for each method to prevent complications. These methods have been studied and proven safe for most pregnant people.
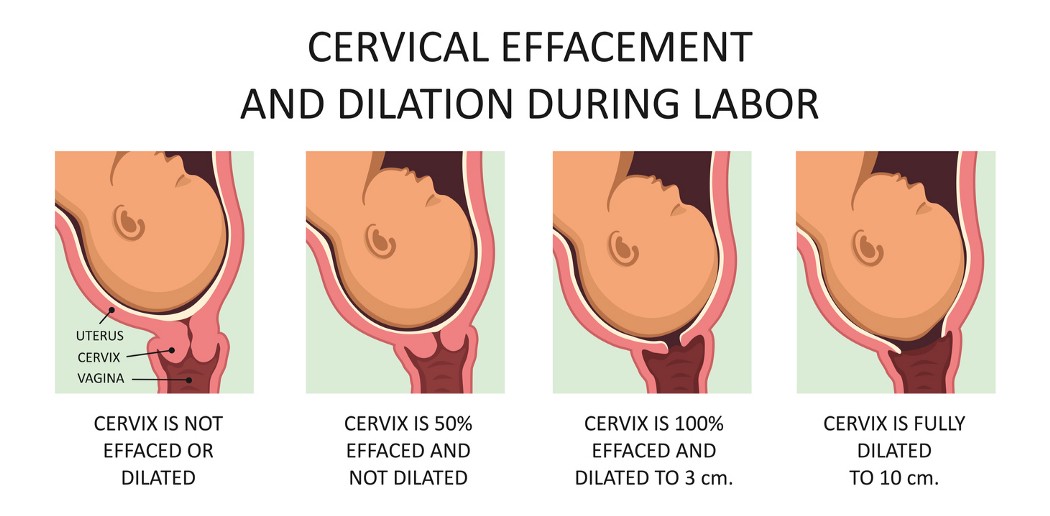
Infographic: Nmfotograf Istock/Getty Images
1. Nipple Stimulation: This isn’t as fun as it sounds! Nipple stimulation releases endogenous oxytocin which causes contractions. Nipple stimulation is best accomplished by applying a mechanical breast pump to both breasts. One problem with this method is once the stimulation is stopped, the oxytocin level drops, and contractions can also stop if labor wasn’t fully established. Time limit: 20 minutes on, 20 minutes off, for up to 2 hours
2. Foley Balloon: Mechanical dilators, like the foley balloon or Cook cervical balloon, put pressure on the cervix, stretch the lower segment of the uterus, and indirectly release cervical softening hormones called prostaglandins. The end of the balloon can be attached to traction to aid in cervical dilation. Once the balloon comes out, the cervix is usually 3–5 centimeters dilated, though contractions will usually need to be stimulated to induce labor. Time limit: 12–24 hours
3. Cervidil or Cytotec: These prostaglandin medications are placed directly behind your cervix to soften the cervix and help thin it out. Cytotec can be taken orally, which is great if the amniotic membranes are ruptured. Though the goal of these medications is to ripen a cervix for labor. Both are capable of producing contractions. Labor is more likely if you have had more than one baby. Time limit: 12 hours for Cervidil; Cytotec is given every 3–4 hours for up to 3–4 doses
4. Pitocin: Pitocin is the synthetic version of oxytocin. It is given through an IV and can be titrated to achieve an adequate contraction pattern. Pitocin is the most common method of induction or augmentation of labor and is rapidly cleared by the body once it is turned off. Pitocin can be given after delivery to prevent uterine atony and postpartum hemorrhage. While in labor, your nurse or healthcare provider will carefully monitor the fetal heart rate and contraction pattern to prevent complications. Time limit: No time limit; postpartum complication risks increase with prolonged exposure (>24 hours) for some people.
Your provider should explain the risks, benefits, and alternatives for any induction process. Each pregnancy is different so the method that worked for your first pregnancy may not be an option for future pregnancies.
Also, unless you have a medical condition validating an induction prior to 39 weeks gestation, your provider cannot induce labor. No matter how bad your back hurts or if your mom is coming in from out of town.
Trust the process and be patient!
Article originally published on Medika Life.









