Laparoscopic Supracervical Hysterectomy; A Faster Return to Normal Life
An Obgyn explains this surgical procedure.
“I want to have a hysterectomy.” Patients, who are sick and tired of heavy bleeding and pelvic pain, often say these words. Any woman scheduled for the surgical removal of the uterus owes it to herself to know that not all hysterectomies are the same. Different surgical techniques lead to different results and recovery times.
This article is part of Medika’s Preparing For series and covers laparoscopic supracervical hysterectomy (LASH) to help a patient properly prepare herself for a procedure. We answer questions about how long the procedure will last, what’s involved, what to expect, and even advice on packing your bag. While your surgeon preps, we’ll make sure you’re ready.
What is a hysterectomy?
A hysterectomy is a surgery to remove the uterus. Hysterectomies are performed for a variety of gynecologic conditions such as uterine fibroids, heavy periods, endometriosis, chronic pelvic pain, uterine prolapse, and gynecologic cancer.
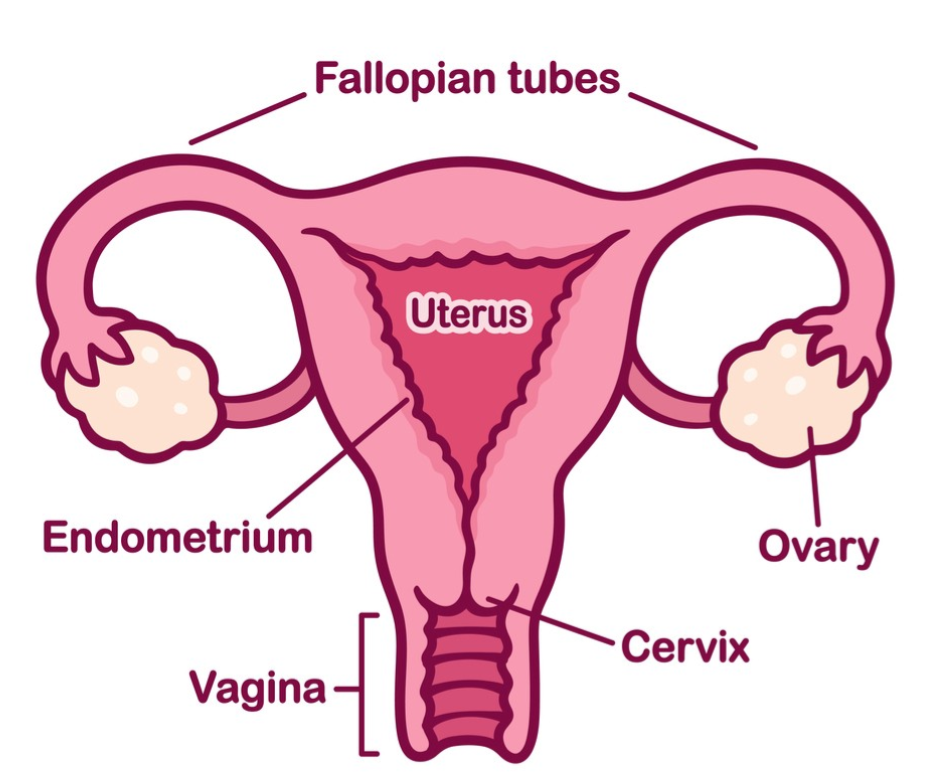
When the entire uterus is removed, this is called a total hysterectomy. If the entire uterus, tubes, and ovaries are removed this is called a total hysterectomy with bilateral salpingo-oophorectomy. Sometimes the uterus is removed, but the cervix is left behind. This surgical technique is called a supracervical hysterectomy.
During hysterectomies, Obgyns often recommend fallopian tube removal (bilateral salpingectomy) to reduce ovarian cancer risk. Some women will also need the removal of the ovaries (oophorectomy). Hormonal changes only occur when the ovaries are removed.
Gynecologists perform hysterectomies through a variety of techniques. The size of the uterus, surgeon experience, the patient’s body type, and the prior surgical history help determine the proper surgical approach. Techniques include:
- Vaginal hysterectomy
- Abdominal hysterectomy
- Laparoscopic hysterectomy (total or supracervical)
- Laparoscopic-assisted vaginal hysterectomy
- Robotic hysterectomy
What are the advantages of laparoscopic supracervical hysterectomy?
Many patients who need a hysterectomy are concerned about a long recovery and missing time off work. A laparoscopic supracervical hysterectomy is an excellent option for hysterectomy candidates who do not have any cervical problems.
The cervix is the opening of the uterus at the back of the vagina. Some women are not candidates for supracervical hysterectomy due to a history of cervical dysplasia, HPV, or abnormal pap smears.
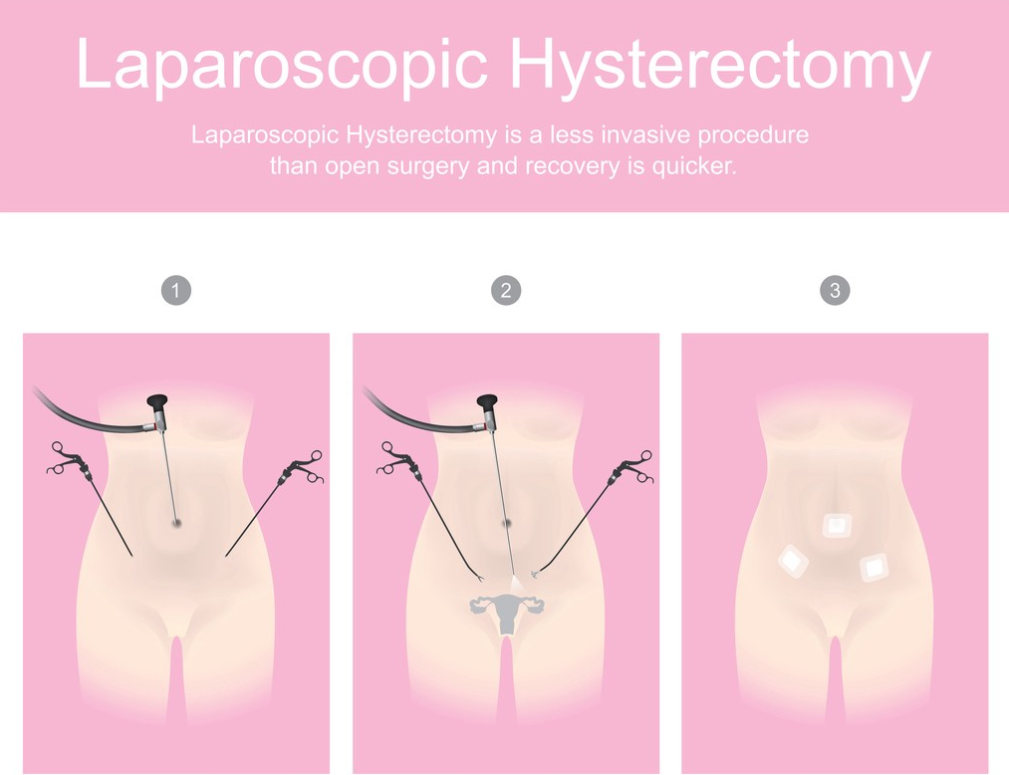
This minimally invasive technique allows faster recovery, reduced pain, and shorter hospital stay. Patients benefit from small incisions, a short hospital stay, and a quicker return to work, exercise, and everyday activities.
During laparoscopic surgery, the surgeon places a camera through the umbilicus (belly button). This technique allows the surgeon to use small instruments to perform the surgery and monitor the surgical field through these tiny incisions.
How long will I be in the hospital?
Surgeons perform a laparoscopic supracervical hysterectomy as an outpatient procedure or inpatient surgery with an overnight stay. Various factors, such as the patient’s underlying health status, surgical complexity, and physician preference, help determine the surgical plan.
Most laparoscopic supracervical hysterectomy patients can leave the hospital much faster after a traditional abdominal hysterectomy.
Can my family visit me?
A trusted family member should drive you to and from the hospital or ambulatory surgery center for a laparoscopic supracervical hysterectomy. Families are welcome to stay with you before and after surgery. Hospital visitor policies for overnight stays vary from region to region due to the Covid-19 pandemic.
Does my procedure require an anesthetic?
A laparoscopic supracervical hysterectomy requires general anesthesia. An anesthesiologist will temporarily put the patient to sleep so they will feel no pain during surgery. The surgeon may also inject a local anesthetic into the incisions to decrease postoperative pain.
What’s the procedure when I check-in?
Most surgeries will involve a preoperative visit with your surgeon to go over the procedure’s risks and benefits in detail. Your surgeon answers questions regarding your upcoming surgery. The surgical consent form is reviewed, signed, or updated with any changes.
Because any hysterectomy will eliminate the possibility of child-bearing, your doctor will ask questions to make sure you are confident you will not want children in the future.
In most settings, patients will receive a preoperative phone call by a nurse or medical assistant one to two days before surgery. If any blood work or preoperative testing is required, it will be scheduled and confirmed.
After arrival at the hospital or Ambulatory Surgery Center, the staff will guide you to the preoperative holding area to change into a surgical gown and store your valuables. You will meet the nursing team who will provide care during your stay. Your nurse will place an IV at this time.
The anesthesia team will come to interview you and answer questions. Typically your surgeon will also come and review any last-minute questions.
What happens on the day of surgery?
Graphic_BKK1979 Istocky by Getty
What happens in the operating room?
After the preoperative evaluation, the team will guide you to the operating or procedure room. You will move from the mobile bed to the operating table. Once you are positioned comfortably and safely, the anesthesiologist will give you medication through your IV to help you go to sleep.
The OR nursing team will cover your body with sterile drapes and prep the abdomen for surgical sterility. The team then performs a “surgical time-out.” The head nurse will read a surgical safety checklist aloud, requiring all surgical team members to be present and attentive.
The gynecologic surgeon will insert a speculum into the vagina to allow visualization of the cervix, the opening of your uterus located at the back of the vagina.
Once the speculum is in place and the cervix visualized, the surgeon inserts a device called a uterine manipulator into the cavity of the uterus. This step facilitates the surgeon’s ability to safely operate and avoid injury to surrounding tissue such as the bladder, rectum, intestines, and ureter.
The surgeon will mark the surgical sites with a small marking pin and insert a small camera through an incision in the belly button. Air inflates and distends the abdomen to allow visualization of the pelvis. My preference is to insert a specialized instrument called Gel point mini by Applied Medical. This type of port enables me to use one incision to perform the procedure.

The surgical team positions the laparoscopic camera to show the pelvic anatomy. We pass small instruments through the additional ports.
Many surgeons recommend complete removal of the fallopian tubes (bilateral salpingectomy) at the time of surgery as this technique reduces the risk of ovarian cancer.
The fallopian tubes are located and grasped with one instrument. Using the other hand, the surgeon clamps and cuts the fallopian tubes from the adjacent anatomy.
The surgeon travels down the sides of the uterus, freeing it from the connecting tissues. The round ligament and uterine/ovarian ligaments are clamped, cauterized, and then cut. At each step, the surgeon will take precautions to control and avoid bleeding.
Critical anatomy lies towards to lower end of the uterus. The surgeon will separate the bladder from the lower uterine segment to allow visualization of the cervix and avoid bladder injury.
The surgeon will focus careful attention on the uterine arteries, the main blood supply to the uterus. These two blood vessels travel over the ureters, which are the tubes connecting the kidney to the bladder.
At this point, we can separate the uterus from the cervix for removal. There are various techniques, but I prefer to use a product called the bipolar Lina Loop.

The surgeon lassos the loop over the uterus and positions it at the uterus and the cervical junction. We perform a safety check to make sure no other anatomy is in contact with the loop. Then the uterus is amputated from the cervix.
The uterus is now free but still needs to be removed. We place the uterus into a surgical bag for tissue retrieval.

The surgeon examines all of the surgical sites for bleeding. When safe, the Obgyn removes the uterus safely located inside the bag through the umbilical (belly button) incision. We removal the operative ports and sew the surgical incisions closed.
Once the procedure is complete, the surgical team completes a post-procedure review. All instruments and equipment are counted and verified. When finished, the anesthesiologist will begin to wake the patient up for transfer to the recovery room.

Monekybusinessimages Istock by Getty
How long will I be in the operating room?
Once the patient enters the operating room, a series of safety steps must occur. This process takes about 20 minutes.
The operative time for laparoscopic supracervical hysterectomy varies. The surgeon’s experience, surgical technique, patient body type, uterine size, and previous surgeries are all factors. For example, a small uterus is a much easier surgery than a large, fibroid uterus.
In general, the patient should expect 1–2 hours of total operative time.
When can I go home?
Postoperative recovery time will vary from person to person. Some surgeons will recommend an outpatient procedure, while others prefer an overnight stay. The patients underlying health status, surgical complexity, and physician preference are all factors.
Each patient must meet specific discharge criteria to be able to go home. The patient’s vital signs must be stable. The patient must be alert, oriented, and able to walk with assistance. The recovery room team will control postoperative nausea, vomiting, and pain and monitor for postoperative bleeding.
The nursing team will go over discharge instructions, and confirm postoperative pain management plans.
What is the usual recovery time?
Most women should be able to return to normal daily activities within a few weeks of surgery. The nursing team will help patients walk and move around a few hours after surgery to reduce blood clots’ risk, improve lung function, and expedite bowel function return.
Most patients will require pain medication like NSAIDs and narcotics for a time. Many experience discomfort in the right shoulder due to air irritating the nerves of the diaphragm.
Light bleeding, spotting, and brown or black discharge is common and expected. Sanitary napkins are safe to use.
What aftercare is required?
You should speak with your physician regarding the resumption of exercise and sexual activity. Most can return to basic activities in one to two weeks. Sexual activity is typically restricted for 6–8 weeks to allow complete healing.
Your doctor will schedule a postoperative examination 1–2 weeks after the procedure to evaluate the incisions.
Danger Signals to look out for after the procedure
You should call your doctor if you experience heavy vaginal bleeding, fevers, severe nausea or vomiting, worsening abdominal pain, or the inability to pass gas.
If you experience heavy bleeding, abdominal or pelvic pain, a fever, or pain that increases over 24 hours, call your physician. After any surgery, contact your physician if you meet any of the following criteria:
- Pain not controlled with prescribed medication
- Fever > 101
- Nausea and vomiting
- Calf or leg pain
- Shortness of breath
- Heavy vaginal bleeding
- Foul-smelling vaginal discharge
- Abdominal pain not controlled by pain medication
- Inability to pass gas
What preparations should I make for aftercare at home?
Laparoscopic procedures require very little postoperative care. Keep the incisions clean and dry. Patients should avoid sexual activity until cleared by their doctor. One may resume a normal diet the day of surgery and begin light exercise the day after the procedure or when you feel ready.
What information should I provide to my doctors and nurses?
It is very important to provide your doctor with an updated list of all medications, vitamins, and dietary supplements prior to surgery. All medication and food allergies should be reviewed. Share any lab work, radiologic procedures, or other medical tests done by other healthcare providers with your surgeon prior to your procedure.
Thank you to BeingWell for publishing this article on Medium.
Blog Author: Dr. Jeff Livingston
Main Blog Photo By: Nensuria Istocky by Getty